Spring 2026 (Volume 36, Number 1)
The Environmental Footprint of Rheumatologic Medications:
What Prescribers Should Know
By Neha Mathur, MD, and Myles Sergeant, MD, FCFP
Download PDF
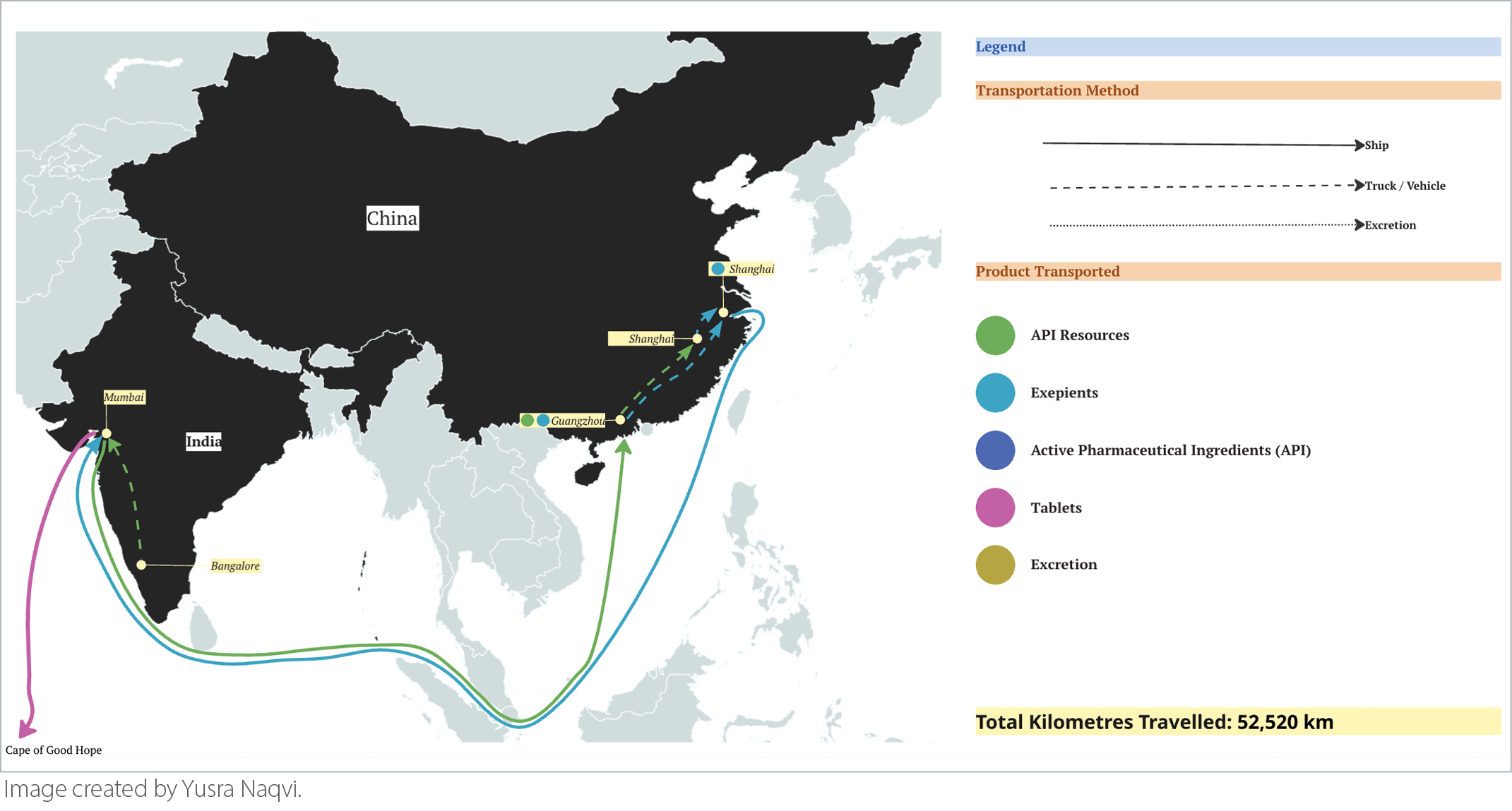
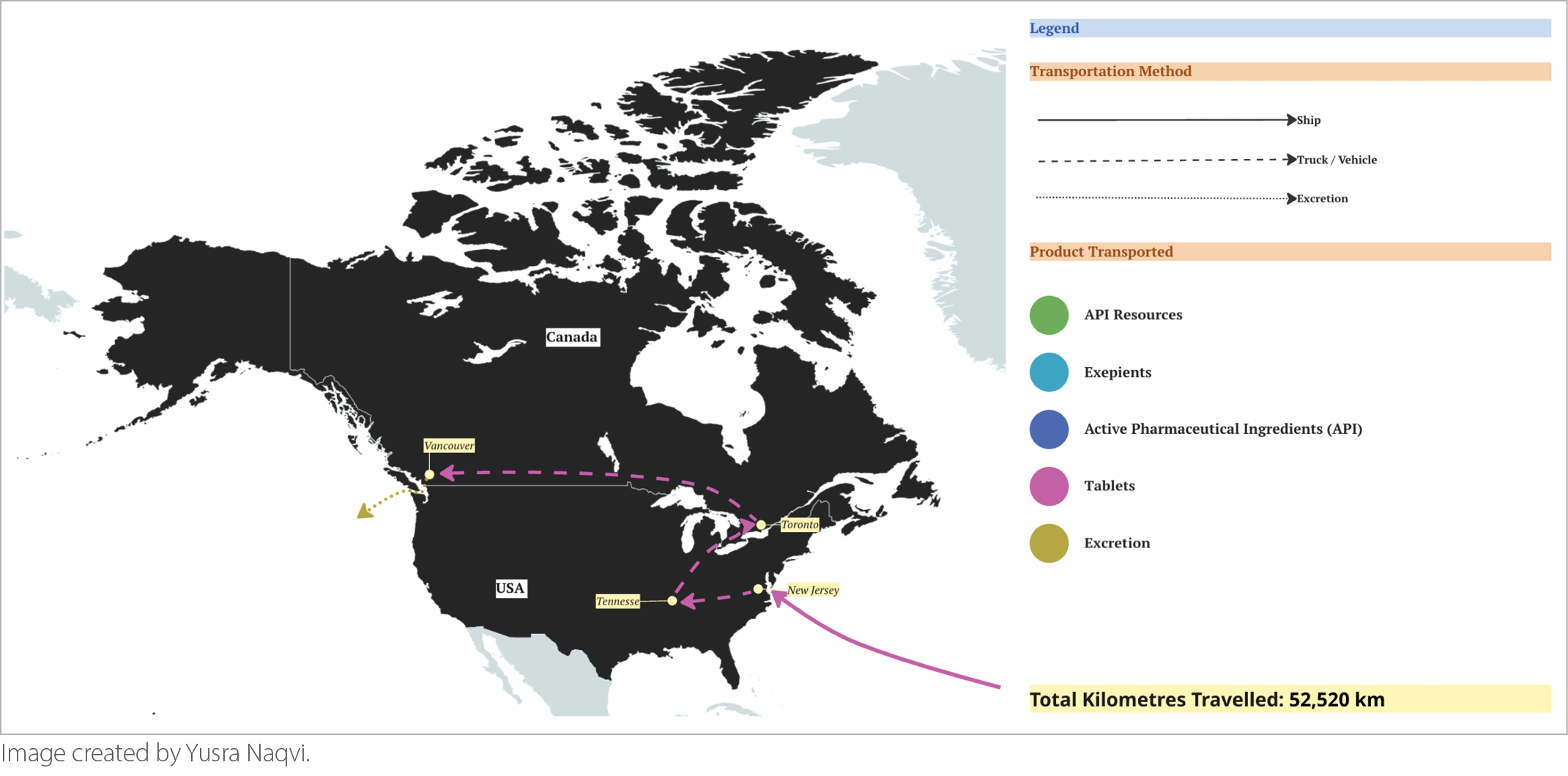
Each and every prescription we provide as physicians carries a hidden journey through the processes of production and supply chains that often span international borders, unknown to patients and providers alike. One example of this is highlighted in our “Journey of a Pill,” which provides a detailed look at the global path of a single pill of clonazepam, a frequently prescribed treatment for various medical conditions such as insomnia, anxiety, and seizure disorders.1 As we follow the path through extraction, manufacturing, shipping, distribution, and elimination, we estimate that each pill commonly travels over 52,000 km before even reaching the patient (Figure 1). This global journey is not unique to clonazepam; it reflects the broader environmental footprint embedded in nearly every medication we prescribe.
Procurement describes the process by which systems acquire essential supplies and services necessary for patient care and represents one of the largest sectors of greenhouse gas (GHG) emissions by the healthcare system. Medications account for around 25% of GHG emissions in healthcare systems, according to assessment by the UK’s National Health Service.2 Pharmaceuticals are inordinately high impact due to the complex supply chains and globalization of manufacturing. Importantly, so‑called “legacy medications” — the drugs we prescribe steadily for years or even decades — often become the most environmentally consequential because their cumulative production and distribution footprints grow over time. This poses a key opportunity for involvement by physicians, as judicious and thoughtful prescribing can meaningfully reduce environmental impact.
Rheumatologic medications have many unique characteristics that may disproportionately increase their environmental impact. For example, patients with rheumatologic conditions are often on legacy therapies, many starting at a young age. Especially early in disease courses, it may take many trials with different medications before finding a stable medication regimen, whether due to non-medical switching, dose adjustments, or fragmented care. When therapies are often long-term and resource-intensive to produce and distribute, prescribing stability reduces unused medication, minimizes cold-chain transport and urgent shipments, and allows supply chains to operate more efficiently. Additionally, the field of rheumatology has seen the rise in use of biologic medications, which include their own unique characteristics when it comes to environmental impact, as they often have high environmental footprints in the manufacturing process. As highlighted in “Sustainable Health Care: An Implementation Guide for Rheumatology,” biologic and targeted synthetic therapies also generate substantial down-stream waste through delivery devices, sharps disposal, and infusion-related consumables.3 This makes waste reduction strategies such as reusable sharps container programs and appropriate medication disposal particularly relevant in this specialty. In addition, thoughtful coordination of medication changes and biosimilar transitions can help avoid parallel prescribing, stockpiling, and unnecessary medication disposal, preserving both environmental and system resources.
Bearing in mind the journey each prescription takes, as prescribers there are many ways we may consciously have an impact on the environmental footprint our care creates. For example, advocating within hospital systems, offices, and pharmacies to carefully consider the impact of the suppliers that are chosen is important. Influencing procurement decisions with the clinical expertise we bring can lead to more sustainable upstream choices. Appraising our own prescribing practices and deprescribing or stably prescribing when clinically appropriate can further reduce waste. Engaging trainees early in their education to instill these concepts can have meaningful downstream effects and lead to a culture shift towards considering sustainability in everyday patient care decisions. Understanding the hidden journey of our medications reminds us that sustainability is not an add‑on to clinical care — it is woven into every prescribing decision we make.
Neha Mathur, MD
Internal Medicine Resident,
Western University
Myles Sergeant, MD, FCFP
Family Physician,
Hamilton Health Sciences and Shelter Health Network
Executive Director,
Canadian Coalition for Green Healthcare
Images created by:
Yusra Naqvi, MSc
Research Assistant,
McMaster University
References:
1. Kaur H, Parascandalo F, Krantzberg G, Ko E, Mathur N, Gill AS, Razack F, & Sergeant M. Journey of a pill. Canadian family physician Medecin de famille canadien. 2025;71(4):263–269. https://doi.org/10.46747/cfp.7104263.
2. Areas of focus. London, UK: National Health Service England. Available at https://www.england.nhs.uk/greenernhs/a-net-zero-nhs/areas-of-focus. Accessed January 29, 2026.
3. Tom S, Barber C, Bernatsky S, Hazel E, Dushnicky M, Baer P, To F, Mendel A, Kaminski J, Sypus A & Waddington K. (2025). Sustainable Healthcare: An Implementation Guide for Rheumatologists. Canadian Coalition for Green Health Care & Canadian Rheumatology Association.
|
-EN-v2.gif)


-EN-v1.gif)
