Winter 2025 (Volume 35, Number 4)
From Polyarthritis to Aggressive Nodulosis: An Unusual Evolution of Rheumatoid Arthritis
By Kavya Mulgund; and Tripti Papneja, MD, FRCPC
Download PDF
|
Case Presentation
A 61-year-old female with hypertension presented initially in 2011 with several weeks of joint pain, morning stiffness and fatigue. Examination demonstrated swelling of multiple metacarpophalangeal (MCP) joints with no extra-articular features. Laboratory testing revealed hemoglobin 88 g/L, ferritin 8 µg/L, ESR 71 mm/hr, CRP 34.8 mg/L, rheumatoid factor 299 IU/mL, and ANA 1:640 speckled. Anti-CCP was negative. She was diagnosed with seropositive rheumatoid arthritis (RA) and was started on methotrexate and hydroxychloroquine with good response. Her RA entered remission by 2013, and she elected to discontinue disease-modifying antirheumatic drug (DMARD) therapy. Between 2013-2024, she was treated for osteoporosis, transitioning from bisphosphonate therapy to denosumab injections. She continued on valsartan and amlodipine for her hypertension. She developed Raynaud’s phenomenon in February 2023.
She was in Pakistan from April to May 2024 and started to feel very unwell with fever, marked fatigue and joint pain/swelling. She couldn’t move her right elbow. She was started on prednisone 60 mg daily, to be tapered by 5 mg every 2 days. In June 2024, she developed nodules on her hands (Figure 1) and reported anorexia with 20 lbs. weight loss, intermittent low-grade fever, cough and xerostomia. Examination detected 6 swollen joints, predominantly affecting MCP and proximal interphalangeal (PIP) joints, and multiple, discrete, tender nodules over the dorsal and palmar aspect of both hands.
Bloodwork showed the following: hemoglobin 114 g/L, WBC 4.1 ×109/L, platelets 219 ×109/L, ESR 40 mm/hr, CRP 1.3 mg/L, persistent ANA ≥1:640 speckled, positive SSA/SSB (>8.0, normal is <1.0), mildly positive RNP (2.0, normal is <1.0), low complement levels (C3 0.80 g/L, C4 0.14 g/L), and negative anti-dsDNA, hepatitis B/C, HIV and Quantiferon gold TB testing. A working diagnosis of RA flare was made, and prednisone and leflunomide were initiated.
|

Figure 1. Papulonodular cutaneous lesions on the hands of our patient.
A punch biopsy of a hand nodule (August 2024) showed dermal proliferation of histiocytes and multinucleated giant cells containing eosinophilic “ground-glass” cytoplasm with sclerotic stroma, confirming the diagnosis of multicentric reticulohistiocytosis (MRH). Biopsy of a lesion on her back was consistent with granuloma annulare.
Given the diagnosis of MRH, malignancy screening was completed. Colonoscopy, mammography and CT scan of the head were normal. CT of the abdomen/pelvis revealed hepatic and renal cysts. CT of the chest showed cystic interstitial lung disease with multiple thin-walled cysts, most consistent with lymphoid interstitial pneumonia. Her pulmonary function test demonstrated restrictive defects. She had an endobronchial ultrasound on November 6th for sampling of mediastinal lymph nodes, results of which are pending. ENT is following her for a 3.7 x 3.0 cm right paratracheal mass, presumed to be due to an enlarged thyroid.
Discussion
Multicentric reticulohistiocytosis (MRH) is a rare, multisystem, class IIb non-Langerhans cell histiocytosis characterized by granulomatous proliferation of the mononuclear phagocyte system. It is marked by destructive polyarthritis and papulonodular skin lesions. Polyarthritis is often the first and most prominent feature, progressing to destructive arthritis and disability. We present a case of MRH and review current literature on its clinical features, diagnostic approach, and management.
Epidemiology
MRH is a rare disease with slightly more than 300 cases reported worldwide. The true incidence and prevalence of this disease is unknown. It predominantly affects Caucasian females in their fifth and sixth decade of life, with a female-to-male ratio of 3:1.
MRH is often associated with autoimmune conditions and internal malignancies. A Mayo Clinic review (1980–2017) of 24 cases reported autoimmune disease in 29%, malignancy in 25%, and five-year survival of 85% (95% CI: 74–100%).2 MRH frequently coexists with autoimmune diseases, including Sjogren’s disease, systemic lupus erythematosus, systemic sclerosis, dermatomyositis, celiac disease, and primary biliary cirrhosis.
While MRH cases have been associated with nearly all types of cancer both solid and hematologic, the most common malignancies observed are carcinomas of the lung, stomach, breast, cervix, colon, and ovary. Whether multicentric reticulohistiocytosis is a true paraneoplastic disorder is controversial, because no consistent type of cancer has been associated with MRH. In addition, as multicentric reticulohistiocytosis is very rare, the association with cancer may be coincidental. Moreover, a correlation between the removal of cancer and the disappearance or improvement of multicentric reticulohistiocytosis has not been established.
Clinical Features
In half of the patients, the first sign of the disease is arthritis. In one quarter, papules and nodules are the first sign. The remainder develop skin and joint manifestations at the same time. The most frequent joint manifestations include symmetric and erosive inflammatory arthritis affecting the hands in a distal predominance, but MRH can also involve the elbows, shoulders, hips, knees and feet, and when left untreated can lead to a progressively deforming and destructive arthropathy including contractures and arthritis mutilans.
Cutaneous lesions usually appear within three years of arthritis onset, as acral yellowish to reddish-brown papulonodules. These lesions most commonly occur on the upper half of the body, especially the face, ears, mucosal surfaces (lips, tongue, gums, nostrils, throat, eyelids), hands, and forearms. They range in size from 1-2 mm to several centimetres in diameter and arise in isolation or in clusters or crops with a cobblestone appearance. Mucosal lesions are present in approximately 50% of cases. The skin lesions may cause destruction of cartilage around the ears and nose. Lesions are usually asymptomatic, but one third of patients complain of pruritus. Periungual papulonodular skin lesions are pathognomonic and often coalesce creating the classic “coral bead” or “string of pearls” appearance. Nodules developed a decade later in our patient from the time of initial joint symptoms.
Common systemic symptoms include fever, malaise, and weight loss, often with elevated ESR, anemia, and hypercholesterolemia.1 Systemic involvement may include pleural or pericardial effusions, cardiac failure, mesenteric lymphadenopathy, and urogenital lesions.3
Around one third show autoimmune serologies (anti-Ro, anti-CCP, ANA). Histopathology reveals lymphohistiocytic infiltrates with multinucleated giant cells containing eosinophilic ground-glass cytoplasm.2 Pathogenesis involves monocyte/macrophage activation and osteoclastic activity.
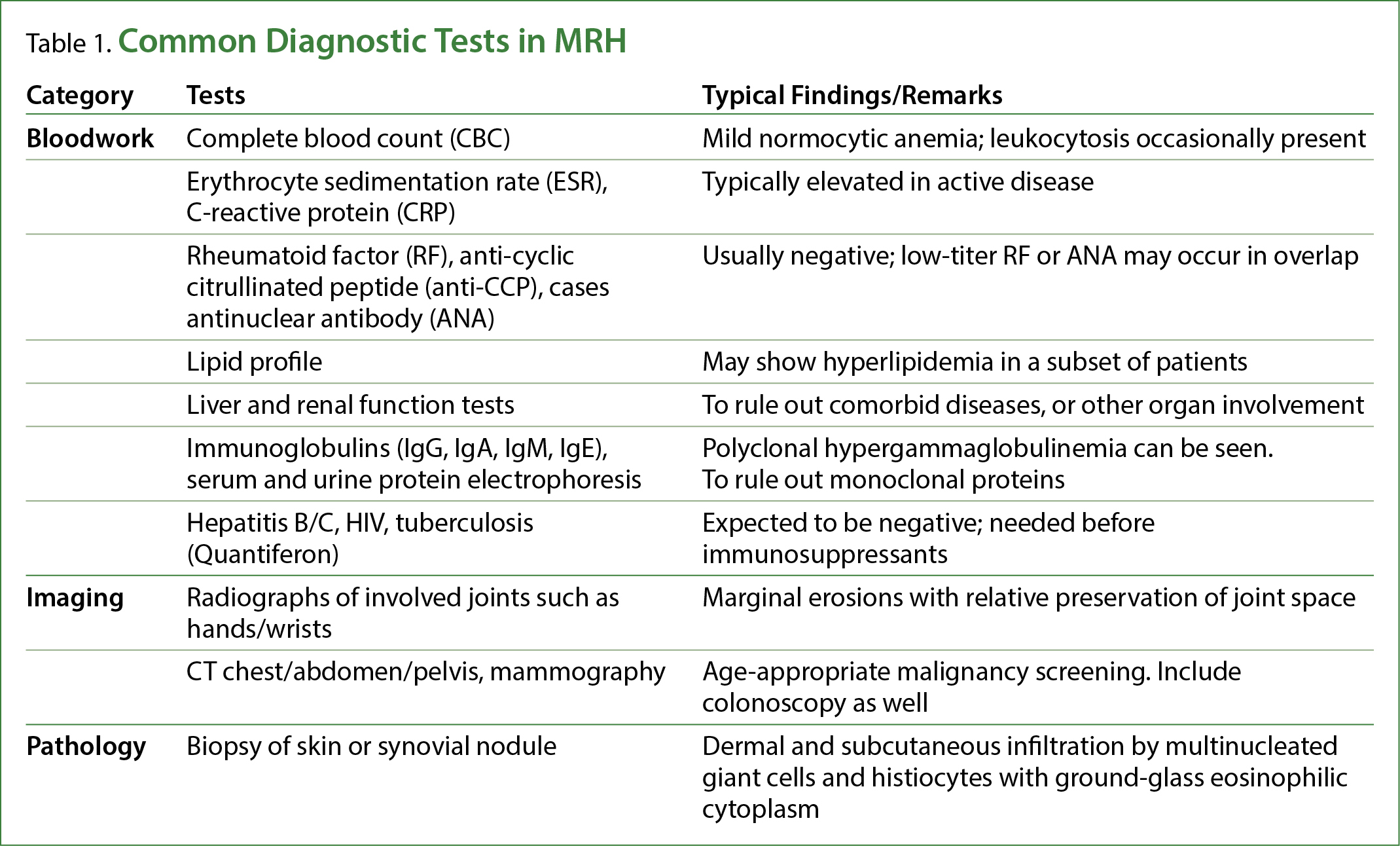
When a case of MRH is suspected, the diagnostic tests in Table 1 should be considered.
Therapeutic Approaches
Treatment aims to control inflammation and prevent joint destruction. Since MRH is a rare disease, there are no standardized treatment guidelines. Therapies include corticosteroids, DMARDs such as methotrexate, azathioprine, cyclosporine, cyclophosphamide, chlorambucil, topical tacrolimus, and rituximab.4-6 Tariq et al. reported methotrexate controlled arthritis in 28% and skin lesions in 38%, while cyclophosphamide achieved complete remission in 20% and partial improvement in 40–45%.7 Anti-TNF agents, anakinra, bisphosphonates, Janus Kinase (JAK) inhibitors (upadacitinib), and tocilizumab are additional options.8
In many patients, multicentric reticulocytosis can go into remission after an average course of 8 years; however, by this time considerable joint destruction may have occurred. Arthritis mutilans may develop in 50% of cases. Patients are left with crippling, deformed joints and a disfigured facial appearance.
Early diagnosis and prompt DMARD therapy are crucial, as MRH often follows an aggressive, erosive course leading to joint destruction if left untreated.
Back to the Case
Despite treatment escalation with prednisone, hydroxychloroquine, leflunomide and methotrexate added in September 2024, she experienced persistent fatigue, arthritis, and progressive nodulosis. In August 2025, adalimumab was initiated. At the time of writing, she has completed eight weeks of adalimumab with no significant improvement in rheumatologic or dermatological symptoms. A change in therapy to tocilizumab is being considered.
Conclusion
MRH is a rare but severe systemic disease with distinctive skin and joint features. Its association with malignancy and autoimmune conditions necessitates thorough evaluation. Early recognition and initiation of immunosuppressive or biologic therapy improve outcomes.
Kavya Mulgund
BHSc student,
Queen’s University
Kingston, Ontario.
Tripti Papneja, MD, FRCPC
Clinician-Teacher,
University of Toronto
William Osler Hospital
Brampton, Ontario
Glossary
ANA: Anti-nuclear antibody
Anti-CCP: Anti-cyclic citrullinated peptide
Anti-dsDNA: Anti-double-stranded DNA
Anti-Ro: Anti-Ro antibodies, also known as anti-SSA/Ro antibodies
CRP: C-reactive protein
ENT: Ear nose and throat specialist
ESR: Erythrocyte sedimentation rate
HIV: Human immunodeficiency virus
RNP: Ribonucleoprotein
SSA/SSB: Sjögren's Syndrome A antibodies/ Sjögren's Syndrome B antibodies
TB: Tuberculosis
WBC: White blood cell
References
1. Ashaolu O, Ng S, Smale S, et al. Multicentric Reticulohistiocytosis–A rare and disabling disease. Clinical Case Reports. 2023;11(9):e7846.https://doi.org/10.1002/ccr3.7846.
2. Sanchez-Alvarez C, Singh Sandhu A, Crowson CS, et al. Multicentric reticulohistiocytosis: the Mayo Clinic experience (1980–2017), Rheumatology. 2020; 59(8):1898-1905. https://doi.org/10.1093/rheumatology/kez555.
3. Mariotti E, Corrà A, Lemmi E, et al. Multicentric Reticulohistiocytosis Associated with an Early Form of Systemic Lupus Erythematosus: A Case Report of a Rare Disease, with Mini Review of the Literature. Journal of Clinical Medicine. 2022;11(21):6529-6529. doi:https://doi.org/10.3390/jcm11216529.
4. Bin FB. Multicentric reticulohistiocytosis in a Malaysian Chinese lady: A case report and review of literature. Dermatology Online Journal. 2009;15(1). doi:https://doi.org/10.5070/d34wm552ck.
5. Liu YH, Fang K. Multicentric reticulohistiocytosis with generalized systemic involvement. Clinical and Experimental Dermatology. 2004;29(4):373-376. doi:https://doi.org/10.1111/j.1365-
2230.2004.01531.
6. Lim K, D’Souza J, Vasquez JB, et al. Looks Can Be Deceiving: A Case Report on Multicentric Reticulohistiocytosis Successfully Treated with Rituximab. Cureus. Published online May 3, 2017. doi:https://doi.org/10.7759/cureus.1220.
7. Tariq S, Hugenberg ST, Hirano-Ali SA, et al. Multicentric reticulohistiocytosis (MRH): case report with review of literature between 1991 and 2014 with in depth analysis of various treatment regimens and outcomes. SpringerPlus. 2016; 5:180. doi:https://doi.org/10.1186/s40064-016-1874-5.
8. Pacheco-Tena C, Reyes-Cordero G, Ochoa-Albíztegui R, et al. Treatment of Multicentric Reticulohistiocytosis With Tocilizumab. Journal of Clinical Rheumatology. 2013;19(5):272-276. doi:https://doi.org/10.1097/rhu.0b013e31829cf32b.
|
-EN-v2.gif)


-EN-v1.gif)
