Spring 2024 (Volume 34, Number 1)
CPD for the Busy Rheumatologist
Mini-Practice Audit Model (mPAM): Overcoming the “Fear” of Chart Audits
By Raheem B. Kherani, BSc (Pharm), MD, FRCPC, MHPE; Elizabeth M. Wooster, M.Ed, PhD(c); and Douglas L. Wooster, MD, FRCSC, FACS, DFSVS, RVT, RPVI
Download PDF
“So, is it as easy as they say to obtain section 3 credits?” inquires Dr. AKI Joint, a rheumatologist member of the Canadian Rheumatology Association (CRA). “I am starting to understand the purpose of the quality improvement cycle with plan-do-study-act (PDSA). It is even starting to make sense how knowledge translation may work in rheumatology, with all the advances that have happened, particularly in immunology. How do I apply this to my practice? I have heard that I could do a chart audit. But does that have to be as involved as the chart audit I did during my CRA Research Summer Studentship as a medical student? It must be more straightforward than that…”
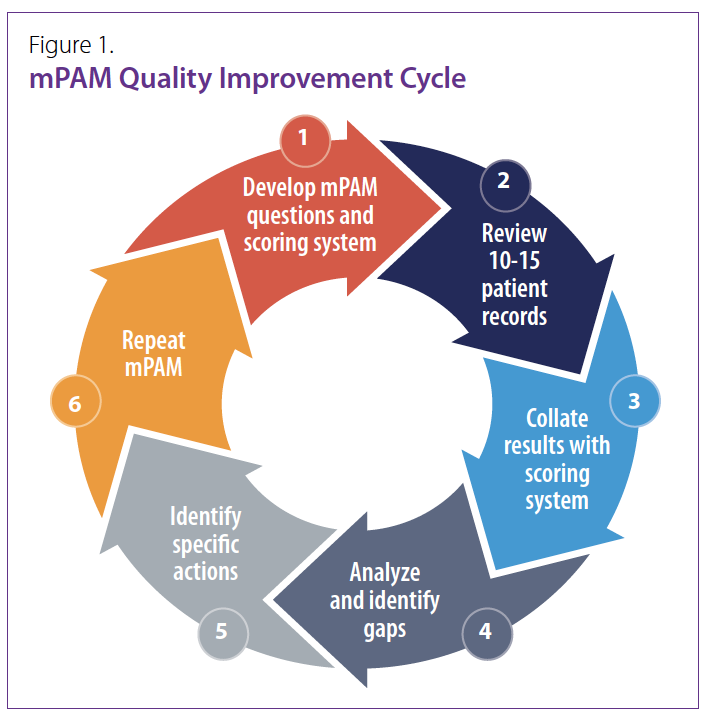
An mPAM (mini-Practice Audit Model) is a focused audit based on individual practice patterns.1 The individual formulates their own questions for their mini-audit. To complete the audit a limited number of patient charts are reviewed, usually 10-15 charts. The scoring system for the review allows objective analysis and identification of any gaps. The gaps can be directly mapped to specific actions (system, knowledge, skills, etc.) to implement guidelines in clinical practice (Figure 1).
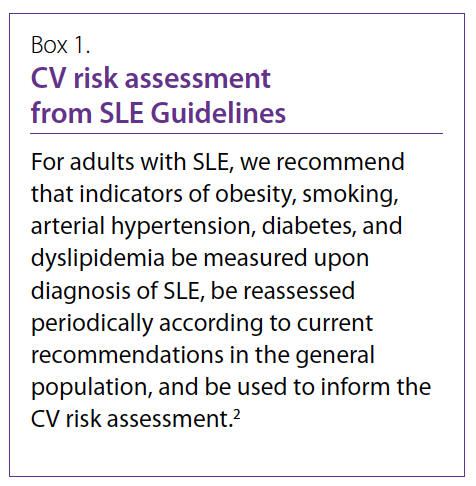
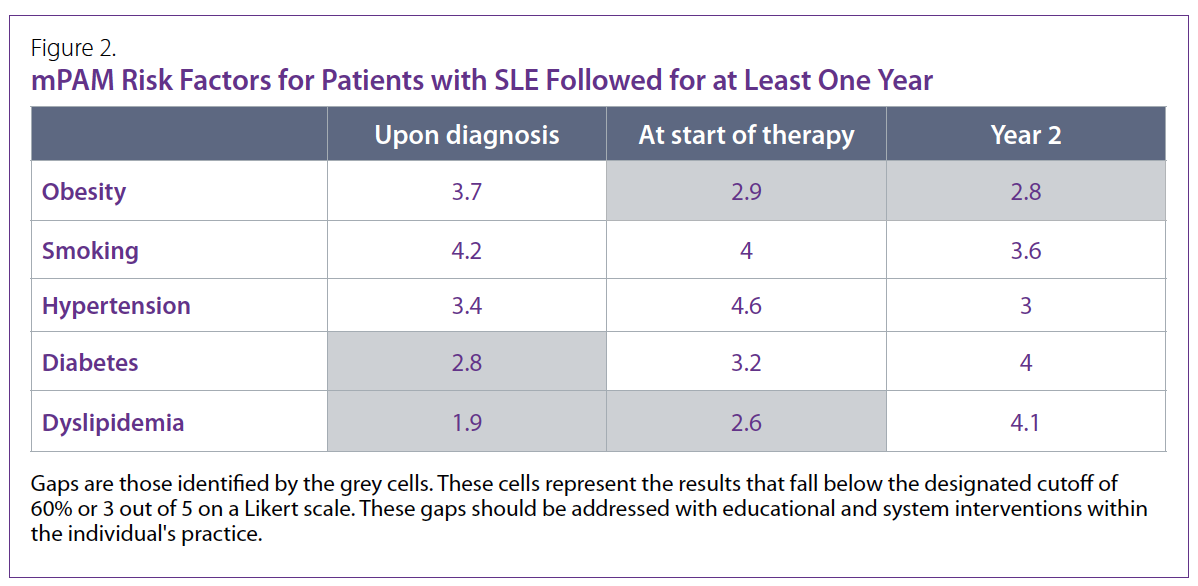
Using the 2018 systemic lupus erythematosus (SLE) Guidelines (Box 1)2, as an example, questions about cardiovascular risk assessment can be the basis of an mPAM. Using a 1-5 Likert scale, the defined questions are assessed. Approximately 10-15 charts are selected, and the results are collated (Figure 2). There is an opportunity to review lipid profiles and other cardiovascular risk assessments more consistently with SLE patients from this audit. Gaps are identified as those cells that fall below the designated cutoff. When using a 1-5 Likert the cutoff is usually 3 or 60%. Educational and system activities are chosen to address the issues underlying the identified gaps. A repeat mPAM is conducted once the remedial activities are completed to determine if the gaps have been addressed. If there is interest in determining long-term improvement, the mPAM process may be repeated at 6-month intervals to determine the impact on patients’ cardiovascular risk assessment as per the 2018 SLE Guidelines.
“So, it isn’t as time-consuming as the chart audit I did during my Summer Studentship,” says Dr. AKI Joint. “I will use this approach every 6 months to actively monitor my implementation of the SLE and other guidelines in my practice (and to get MOC Section 3 credits)”3,4
Raheem B. Kherani, BSc (Pharm), MD, FRCPC, MHPE
CRA Education Committee Past Chair,
Program Director and Clinical Associate Professor,
University of British Columbia
Division Head, Rheumatology, Richmond Hospital
Clinician Investigator, Arthritis Research Canada
Rheumatologist, West Coast Rheumatology Associates
Richmond, British Columbia
Elizabeth M. Wooster B.Comm, M.Ed, PhD(c)
OISE/University of Toronto
Research Associate,
School of Medicine, Toronto Metropolitan University
Douglas L. Wooster, MD, FRCSC, FACS, DFSVS, RVT, RPVI
Professor of Surgery,
Temerty Faculty of Medicine, University of Toronto
References:
1. Wooster DL. A Structured Audit Tool of Vascular Ultrasound Interpretation Reports: A Quality Initiative. Journal for Vascular Ultrasound. 2007; 31(4):207-210. doi:10.1177/154431670703100404.
2. Keeling SO, Alabdurubalnabi Z, Avina-Zubieta A, et al. Canadian Rheumatology Association Recommendations for the Assessment and Monitoring of Systemic Lupus Erythematosus. J Rheumatol. 2018 Oct; 45(10):1426-1439. doi: 10.3899/jrheum.171459. Epub 2018 Sep 1. PMID: 30173152.
3. Kherani RB, Wooster EM, Wooster DL. MOC Section 3 Credits: These Can Be Easy. CRAJ. Fall 2023; 33(3): 20.
4. Kherani RB, Wooster EM, Wooster DL. Knowledge Translation: What’s in It for Me? CRAJ. Winter 2023; 33(4): 22-23.
|




