Summer 2019 (Volume 29, Number 2)
A Snapshot of Access to Rheumatology Tests in Canada
By Dr. Shirley Lake, on behalf of the CRA Choosing Wisely sub-committee
Download PDF
Over the past several years, ordering certain medical
tests and treatments has become more restricted. The
Canadian Rheumatology Association (CRA) sent out a
survey this spring to understand how this has impacted rheumatologists
across the country. Thanks to the 132 respondents
(approximately 22% of the membership), we have learned that
there is a lot of variability in how these tests can be accessed
both between and within the academic and community practice
settings in different provinces. Furthermore, restrictions are often
site-specific and don't apply to the province as a whole.
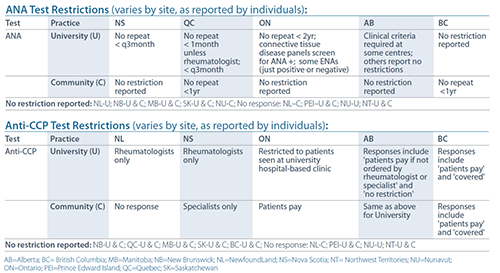
The anti-nuclear antibodies (ANA) test and anti-cyclic citrullinated
peptide (CCP) test were identified as examples of
this variation. ANA tests could be restricted in how frequently
they could be ordered, anywhere from every month to every two
years. One province had restrictions on ANA testing based on
clinical criteria. Anti-CCP tests were restricted in many provinces,
in that it was not accessible unless the patient paid for
the test. In some provinces the test could only be ordered by a
rheumatologist or other specialist.
An abridged version of the survey results for these two tests
is shown below. The complete data table showing all provinces and territories can be viewed by clicking here.
There were many interesting comments from the membership.
One common theme was that some restrictions are
appropriate, as certain tests were not evidence based such as
bone scans for inflammatory arthritis. There were comments
about the most effective means of decreasing inappropriate
testing, whether education may be more effective than restriction,
or allowing only specialists to order some tests, such as
human leukocyte antigen B27 (HLA-B27) and anti-neutrophilic
cytoplasmic antibodies (ANCA). Another comment was
that, although there is inappropriate lab testing, it is not as
high impact as inappropriate imaging or procedures such as
magnetic resonance imaging (MRI) for knee osteoarthritis or
arthroscopic surgery for osteoarthritic knees.
With increasing demands on health care, and an unsustainable
rise in heath spending, the CRA should help guide
the development of additional cost-effective strategies, while
continuing to maintain the highest level of care for our patients.
More evidence on the best strategies for ordering these
tests may help standardize care across Canada to ensure the
highest quality care that is effective, efficient, equitable, timely,
safe and patient centred.
For complete access to the survey data on restricted tests
(anti-nuclear antibodies (ANA), extractable nuclear antigen
(ENA), erythrocyte sedimentation rate (ESR), vitamin D, anti-CCP, ANCA, aspartate aminotransferase (AST), HLA-B27,
bone mineral density (BMD), arthroscopic knee debridement,
hyaluronic acid injection, bone scans, MRI, and others) please
visit craj.ca. We also welcome any updates or corrections to
this information, as it is based on respondent knowledge/
experience and may not fully reflect the current situation in
a certain province or practice setting. These can be sent to
sranta@rheum.ca.
To view the complete data table showing all provinces and territories, click here.
|




