Fall (Volume 28, Number 3)
Choosing Wisely Canada:
Clinical Audit of ANA Ordering Patterns in Community Rheumatology Referrals
By Nadil Zeiadin, MD, CM, FRCPC; Henry Averns, MB, ChB, FRCP (Lond), FRCPC
Download PDF
Anti-nuclear antibodies (ANA) can be found in the sera of many patients with rheumatic and non-rheumatic conditions, as well as in healthy people. While the average sensitivity of ANA in patients with systemic lupus erythematosus is 93%, up to 20% of healthy people will also test ANA positive.1 Consequently, the testing of these autoantibodies must be done in the right clinical context, to avoid both unnecessary testing and erroneous interpretation of results.1-3
Members of the Canadian Rheumatology Association (CRA) recently identified ANA as a test that was often inappropriately ordered in adults.4 This can result in further unnecessary testing, erroneous diagnosis or even inappropriate therapy.1 As well, unnecessary testing of ANA contributes further to the growing Canadian healthcare budget, which was estimated to reach 11.5% of the gross domestic product (GDP) in 2017.5
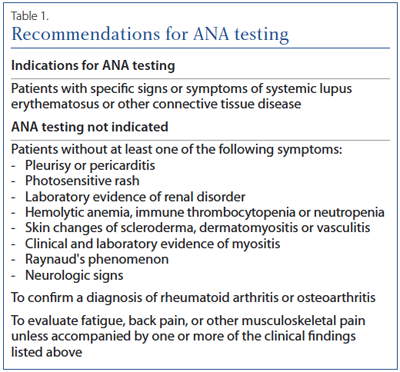
In an effort to decrease unnecessary testing, the CRA published recommended indications for ANA testing in 2015 as part of the Choosing Wisely Canada campaign.4 These recommendations were in keeping with guidelines published in 2013 by the Government of British Columbia (BC).6 Principally, the recommendations outline that ANA testing should be ordered only if the clinician feels there is a reasonable clinical suspicion of systemic lupus erythematosus (SLE) or connective tissue disease (CTD) based on historical information, physical findings, and results of other laboratory tests. While recommendations aim to reduce the frequency of ANA testing, they have been shown to carry a very low risk of missing an underlying case of CTD.7
Since the publication of the Choosing Wisely recommendations two years ago, we have sought to evaluate the ANA ordering patterns within our local referral network, composed primarily of general practitioners. Additionally, we wanted to identify how often a positive ANA result triggered a rheumatology referral. Lastly, we assessed whether raising awareness of published recommendations would alter ANA ordering patterns within our community.
Methods:
We conducted a retrospective chart review of consecutive new referrals received using a convenience sampling method. We excluded referrals sent for a second opinion, repeat referrals or referrals for a specific procedure (e.g. joint injection). We determined from the information provided in the referral whether an ANA was indicated based on published Choosing Wisely criteria and BC recommendations (Table1). We also determined if the clinical question pertained specifically to a positive ANA, and thus, triggered the referral. Following our baseline data, we mailed an information pamphlet highlighting the published Choosing Wisely and BC recommendations regarding ANA testing to offices of general practitioners (GPs) in the surrounding community. We also conducted two in-house educational sessions for community GP’s and nurse practitioners covering the same information as the pamphlets. We subsequently repeated our baseline analysis on a second independent sample of referrals received approximately two months following our intervention.
Results:
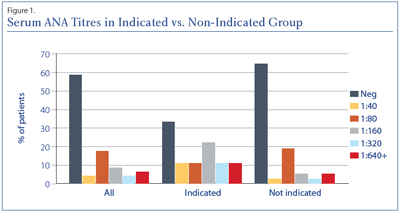
We reviewed 100 consecutive new referrals from October 2016 to March 2017. Forty-six per cent (46%) of referrals had an ANA measured. Of these, 81% did not meet the recommended indications for ANA testing. Of the ANA’s done without an indication, 59% were negative compared to only 33% of the indicated ANA’s (Figure 1). Twenty percent of referrals were requested primarily for interpretation of a positive ANA. Of these, 13 (65%) had an ANA test that was not indicated.
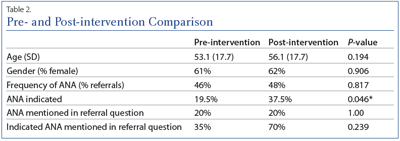
Following our intervention, we reviewed 50 consecutive new patient referrals using the same parameters as our initial sample. We found no significant difference in frequency of ANA testing; however, a significant improvement in the proportion of ANA’s meeting indications for testing was noted (Table 2). There was no significant difference in the number of referrals for positive ANA, but again an overall trend towards improvement in adherence to recommended indications for ANA testing was observed.
Conclusion:
We found serum ANA is frequently ordered among patients referred for rheumatology consultation. Despite published recommendations, we found that the majority of ANA testing is not indicated. This is consistent with results from other Canadian sites8 and the U.S.9 Apart from contributing to healthcare costs, we found that a large proportion of unnecessary ANA tests will also result in referral to the rheumatology clinic. This is of concern as access to rheumatologists is already limited within many parts of Canada, with wait times for patients with suspected rheumatic disease exceeding established benchmarks.10
With respect to reducing unnecessary ANA ordering, we found that raising awareness regarding the Choosing Wisely recommendations produced a significant reduction in the proportion of inappropriate ANA testing among our referrals. Nonetheless, there was no reduction in the frequency of ANA’s ordered or the number of referrals for positive ANA. We suspect that this is most likely due to primary providers ensuring that they list an accepted indication within their referrals rather than ordering ANA less frequently. Thus, although further education for the use of ANA should be part of our strategy, a varied approach is likely required. Similar educational interventions have been successful to reduce the rate of unncessary ANA testing among rheumatologists.11 Other strategies, such as a laboratory algorithm for ANA testing, have also proven successful8 and should be considered. It is nonetheless clear that inappropriate ANA testing remains a common issue in rheumatology referrals and further research regarding both causes and effective intervention strategies is needed.
Limitations of our study include potential for observer bias. As well, conclusions regarding the intervention effect are limited due to lack of controls and potential for Hawthorne effect.
References:
1. Solomon D, Kavanaugh A, Schur P, Guidelines A. Evidence‐based guidelines for the use of immunologic tests: Antinuclear antibody testing. Arthritis Care Res 2002; 47(4):434–44. doi:10.1002/art.10561.
2. Wiik A, Cervera R, Haass M, et al. European attempts to set guidelines for improving diagnostics of autoimmune rheumatic isorders. Lupus 2006; 15(7):391–6. doi:10.1191/0961203306lu2322oa.
3. Agmon-Levin N, Damoiseaux J, Kallenberg C, et al. International recommendations for the assessment of autoantibodies to cellular antigens referred to as anti-nuclear antibodies. Ann Rheum Dis 2014;73(1):17–23. doi:10.1136/annrheumdis-2013-203863
4. Chow, Thorne C, Bell, et al. Choosing Wisely: The Canadian Rheumatology Association’s List of 5 Items Physicians and Patients Should Question. The Journal of Rheumatology. 2015; 42(4):682–9. doi:10.3899/jrheum.141140.
5. Canadian Institute for Health Information (CIHI). National Health Expenditure Trends, 1975 to 2017. November 2017.
6. BC Guidelines. Antinuclear antibody (ANA) testing protocol [Internet]. 2013 June
7. Ferrari R. Evaluation of the Canadian Rheumatology Association Choosing Wisely recommendation concerning anti-nuclear antibody (ANA) testing. Clin Rheumatol 2015; 34(9):1551–6.
8. Man A, Shojania K, Phoon C, et al. An evaluation of autoimmune antibody testing patterns in a Canadian health region and an evaluation of a laboratory algorithm aimed at reducing unnecessary testing. Clin Rheumatol 2013; 32(5):601–8. doi:10.1007/s10067-012-2141-y
9. Abeles A, Abeles M. The clinical utility of a positive antinuclear antibody test result. Am J Medicine 2013; 126(4):342–8.
10. Widdifield J, Bernatsky S, Thorne J, et al. Wait times to rheumatology care for patients with rheumatic diseases: a data linkage study of primary care electronic medical records and administrative data. CMAJ Open 2016; 4(2):E205–12. doi:10.9778/cmajo.20150116.
11. Lesuis N, Hulscher M, Piek E, et al. Choosing Wisely in Daily Practice: An intervention study on antinuclear antibody testing by rheumatologists. Arthrit Care Res 2016; 68(4):562–9.
Nadil Zeiadin, MD, CM, FRCPC
Rheumatologist,
Southlake Regional Health Centre
Newmarket, Ontario
Henry Averns, MB, ChB, FRCP (Lond), FRCPC
Consultant Rheumatologist
President,
Ontario Rheumatology Association
Kingston, Ontario
|




