Spring 2017 (Volume 27, Number 1)
Imaging of Spondyloarthritis – What Does the Rheumatologist Need to Know?
By Walter Maksymowych, FRCPC
Download PDF
Case: The patient was a 23-year-old male who was referred because of a 3-year history of back pain after lifting heavy equipment during his work as a framer. After his acute pain had resolved, he continued to complain of lower-back and left-buttock pain to the point that he was unable to return to work and reported a claim to the Workers Compensation Board (WCB). His family physician had ordered a B27 analysis, which was positive, and pelvic and lumbar spine radiography, which were reported as normal. The WCB physician had additionally ordered pelvic and lumbar spine magnetic resonance imaging (MRI). The former was reported to have “nonspecific bone contusion” in the left iliac bone on a “water-sensitive sequence” while the T1-weighted spin echo (T1W-SE) had “non-specific sclerosis”.
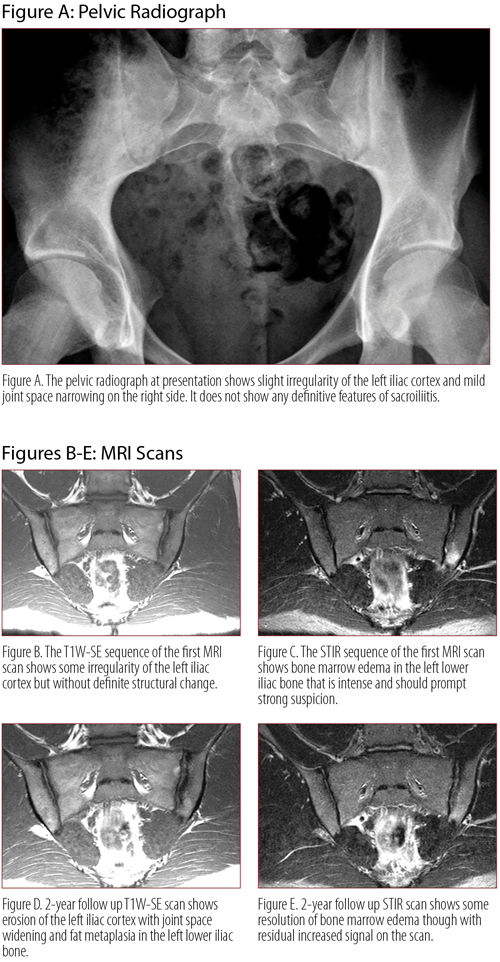
Two years later, the patient is still drawing disability benefits for what is considered back pain related to an injury sustained at work. With the referral from the WCB, a repeat pelvic radiograph reported “slight irregularity of the left iliac cortex in the left sacroiliac joint (SIJ) and mild, non-specific joint space narrowing on the right side”. A repeat pelvic MRI was also ordered and reported as being unremarkable.
The patient described back and right-buttock symptoms that felt worse when rising from bed, morning stiffness of an hour’s duration, symptoms exacerbated by activity but also not alleviated by rest. He had been awakening in the early hours of the morning with back pain and stiffness and no alleviation of his symptoms with over-the-counter ibuprofen and naproxen, or anti-inflammatory agents prescribed by his family physician. However, he was unable to tolerate these medications for more than a few days due to gastric upset. His medical history noted only a 4-pack-years history of smoking. The physical exam showed only mild muscular tenderness in the lower lumbar spine. C‑reactive protein was normal.
Review of both pelvic MRI scans in the context of this clinical presentation indicated a diagnosis of spondyloarthritis (SpA) with MRI features being more typical on the first scan (figures B and C). The scans were reviewed with the patient, and he was informed that the onset of his condition at the same time as his job-related back strain was coincidental, not causal, but a reflection of the typical presentation of this condition in the third decade of life. Since his Bath Ankylosing Spondylitis Disease Activity Index (BASDAI) score was 6.9 and he was intolerant of nonsteroidal anti-inflammatory drug (NSAID) therapy, he was offered treatment with a tumor necrosis factor inhibitor. He was advised to discontinue smoking as this would impair his response to treatment. Four months after treatment, his symptoms subsided, his BASDAI score was 2.6, and he returned to work.
MRI of the SIJ is a major advance in the field because it not only detects inflammation soon after disease onset but may also depict a variety of structural lesions, even without radiographic changes of sacroiliitis. Routine clinical evaluation combines information visualized simultaneously on two types of MRI scans. The T1W-SE sequence detects signal from fat, so adult bone marrow of iliac and sacral bones is bright due to its fat content. The signal from fat can be suppressed to allow visualization of inflammation in the bone marrow using fat-suppressed sequences, such as short tau inversion recovery (STIR), which is also a water-sensitive sequence. Bright signal on the STIR sequence therefore indicates water-related to edema and cellular infiltration associated with inflammation. Cortical bone is dark on both sequences. Both sequences should be routinely ordered as part of a SpA-specific imaging protocol for MRI, and a printout for the radiology department can be downloaded from the Imaging Portal at www.carearthritis.com.
When the possibility of SpA is considered on clinical grounds, when major treatment decisions are at stake, when objective evidence will be essential in changing the patient’s understanding of their illness, and where routine reporting of findings on radiographic imaging is negative and/or non-committal, the rheumatologist is called upon to order and evaluate MRI. Radiography of the sacroiliac joints, a third-world tool for diagnostic evaluation of this condition, is unreliable in early disease and reliance on radiography is a primary factor in delayed diagnosis. It is incumbent on the rheumatologist to learn the language of MRI and to understand basic aspects of interpretation of Digital Imaging and Communications in Medicine (DICOM) images in order to engage in an informed dialogue with the radiologist. Radiologists receive little or no training in the interpretation of MRI features in SpA and are often unaware of the key clinical scenarios where MRI may change the management of patients with SpA.
An online training module based on the DICOM image format is available through the Imaging Portal at CaRE Arthritis (www.carearthritis.com) to provide rheumatologists with essential basic knowledge on MRI interpretation of SpA and other conditions that often fall under the differential diagnosis. A simplified DICOM image-viewing tool allows intuitive learning in how to set up a DICOM image. Each of the 20 cases is highly annotated and experience with MRI interpretation is rapidly acquired through experiential learning, a proven way to acquire new skills. The module is based on the seven years of experience that I and colleagues in musculoskeletal radiology have acquired in providing hands-on training workshops to rheumatologists and radiologists all over the world. Workshop participants have often reported the satisfaction of having acquired a new skill through this experiential learning technique. Maintenance of skills is reinforced through presentation of case-of-the-month content based on images submitted to the Imaging Portal for second-opinion review.
MRI has an indispensable role in the management of patients with SpA and the rheumatologist who is not familiar with basic interpretation of MRI cannot be practising to standard. It is not appropriate or realistic to transfer sole responsibility for interpretation to the radiologist. The presented case illustrates the potential consequences of this strategy.
Walter Maksymowych, FRCPC
Professor of Medicine,
Department of Medicine,
Division of Rheumatology,
University of Alberta
Edmonton, Alberta
|