Summer 2016 (Volume 26, Number 2)
The 2016 Practice Reflection Awards
Download PDF
Gold Award
Henry Averns, MD, FRCPC
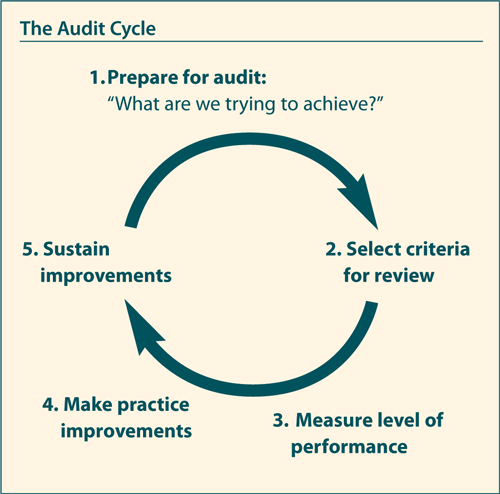
Clinical audit is a process that seeks to improve patient care, processes, and outcomes by measuring one’s care against explicit criteria. This sort of practice reflection is a key pillar of clinical practice; examples of such questions might include:
• “Do I record core spondyloarthritis outcomes clearly in the chart?”
• “Am I asking patients about their immunization status?”
• ”Can I locate this data in the Electronic Medical Record (EMR)?”
• “Do we consider bone sparing therapy in our patients on glucocorticoids?”
In the UK, National Health Services (NHS) clinical audit became a compulsory activity back in 1989. I remember well as a junior doctor the annual audit of quality of medical charts, where one learnt to one’s chagrin that clinical notes were often incomplete, illegible, and fell below the agreed standard. It is often a humbling experience to be reminded of one’s deficiencies in practice. As the culture of reflection and clinical audit developed, the British Society for Rheumatology (BSR) became actively involved, encouraging members to choose from a range of potential audits, and dedicating time at academic meetings to present results of audits to share best practice.
Over the last few years the CRA has recognized that a self-regulating profession must be seen clearly to engage in reflection and practice change. Clinical audit is not simply a process of data collection, not just a survey of one’s practice. It runs far deeper and involves honest reflection on how one is doing, with the opportunity to develop
practice changes which improve overall patient care.
The CRA aims to develop a “library” of potential audit projects, which will include the background data which informs the chosen audit standard, and data-collection forms to allow busy clinician to quickly adopt this in to their practice. As we mature in the process, we will explore electronic media as a tool to improve the efficiency of data collection and review. At this point we need your help. We are seeking champions in each province (including trainees) to drive this process forward. There are no sticks—only carrots. Section 3 credits can be claimed for this activity. Whether the Royal College will mandate this activity in the future remains to be seen, but it is my belief that if we can show all stakeholders that this is an activity which we embrace and perform, the advantages will be self-evident. The Practice Reflection Award is one way in which the CRA is encouraging us all to make clinical audit not just an add-on, but a firm component of our practice.
Silver Award
Philip A. Baer, MD, FRCPC, FACP; and J.P. Raynauld, MD, FRCPC
Forty years ago, smoking in public was quite acceptable, and the dangers of second-hand smoke largely unknown. Philip remembers joining the Non-Smokers Rights Association to try to effect change. The present situation is much improved, but 20% of Canadians still smoke. The dangers are well-known, but the impact on rheumatic
diseases is just beginning to be better appreciated.
Interestingly, a pioneering study on the negative impact of smoking on disease outcomes in ankylosing spondylitis (AS)1 was published 20 years ago by our own Dr. Henry Averns. Dr. Averns has the distinction of being the first winner of the CRA Practice Reflection Award in 2015, and winning the Gold Award again this year. His work helped inspire our Practice Reflection contribution.
Building on multiple studies illustrating the negative impact of smoking on the risk of development, progression, and response to therapy in inflammatory rheumatic diseases presented at European League Against Rheumatism (EULAR) and American College of Rheumatology (ACR) in 2014, we participated in developing a Continuing Medical Education (CME) program on this topic. With the increasing need for chart-audit resources to help rheumatologists fulfill their requirements for Section 3 Royal College MAINCERT credits, we decided to leverage this ENVISION CME program into a chart audit program. Our team included Dr. Shelly Dunne and Dr. Marie-Anais Rémillard, as well as May Shawi, PhD, Ms. Alana Lamb, and Ms. Lise Troyer.
The end product includes an online physician demographic questionnaire, followed by a chart audit of 10 rheumatoid arthritis (RA) patients who are current smokers. Participants then review the ENVISION CME program either online or at a CME event. One to two months later, they repeat the chart audit on 10 more patients, and the results are compared. We are interested in the frequency that smoking status is recorded, the disease activity and functional status of the patients, whether the negative impact of smoking on RA is discussed, and whether
smoking cessation counselling and tools are provided.
Participants receive three Section 3 credits, equivalent to nine credit hours, a significant fraction of the total 25 hours required every five years. We aim to recruit 50 rheumatologists and review 1,000 patients. A preliminary poster covering 11 rheumatologists and 70 patients was presented at CRA 2016. Future plans include updated abstracts at the 2016 EULAR and ACR meetings, as well as a publication submission and possible extension of the audit to patients with AS and psoriatic arthritis (PsA).
Our team thanks the CRA and the Award Selection Committee for recognizing our project. If you are interested in participating in the audit, please visit www.envisionchartaudit.com.
Reference
1. Averns HL, Oxtoby J, Taylor HG, et al. Smoking and outcome in ankylosing spondylitis. Scand J Rheumatol 1996; 25(3):138-42.
Bronze Award
Robert Ferrari, MD, MSc, FRCPC, FACP
I would like to thank the CRA, and in particular the Education Committee, for this brainchild that recognizes the importance of practice reflection. It is clear that practice audits are useful. They improve practice efficiency and effectiveness, reduce clinical errors, demonstrate quality care to stakeholders, promote high standards of practice, lower the risk of liability, and foster practice change. In my submission for the 2016 Practice Reflection Award, however, I also emphasized the additional importance of practice audits as a source of publications. Developing publications has markedly improved my skills in many areas of research design (scholar), writing (communicator), clinical practice (professional), and team effort (collaborator). My submission for this Award was an explanation of how I undertake practice audits, with the a priori view that I would be publishing the results. In my view, a good researcher is also a good practice auditor. I reviewed the step-by-step process of planning a practice audit as if one is planning a research project. I gave two examples in my submission: The design of a practice audit that led to a publication on osteoporosis in men1 and another audit that addressed the prevalence of hyperparathyroidism in fibromyalgia.2 I learned a lot from these audits and the publications hopefully shared some of that knowledge.
The reality is that our practices are loaded with data—if one thinks about a practice audit as an effort to publish results of a data analysis, one can plan the practice audit by going through all the steps described and necessary for a research publication. Imagining a research paper with a clear research question, introduction, and methodology is a good test of how ready the clinician is to conduct a practice audit that will lead to meaningful results. By thinking about practice audits as research projects with the goal of publication, the clinician becomes a researcher, and is far more likely to have a
useful audit.
References
1. Ferrari R. Prevalence of osteoporosis in men aged 65-75 in a primary care setting. A practice audit after application of the Canadian 2010 guidelines for osteoporosis screening. Clin Rheumatol 2015; 34(3):523-7.
2. Ferrari R, Russell AS. Prevalence of primary hyperparathyroidism in a referred
sample of fibromyalgia patients. Clin Rheumatol 2015; 34(7):1279-83. |


